
Texas Children’s leaders share how they are celebrating the holiday safely this year. Read more
Texas Children’s leaders share how they are celebrating the holiday safely this year. Read more
I, Mark Wallace, want to share some exciting news with you. After months of diligent work by our COVID Vaccine Task Force and our hospital leadership, we have received confirmation that Texas Children’s is pre-positioned to receive a shipment of the COVID-19 vaccine next week, which has been produced and tested by Pfizer, and submitted for emergency use approval by the Food & Drug Administration.
This is a tremendous development in the fight against this pandemic. I can think of no greater challenge we have had to overcome together, and I can think of no better news to hear than that Texas Children’s will be given such a vital tool in combating this highly infectious disease.
There are many vaccines on the horizon – Moderna, Johnson & Johnson, AstraZeneca and our own Center for Vaccine Development – but nothing prevents us from following appropriate safety guidelines. Please ensure you and all those around you – both at home and at work – wear a mask properly and over the nose, maintain social distancing at a minimum of 6 feet and practice hand hygiene throughout the day. For on-site meetings, please be sure to adhere to the identified COVID capacity for each meeting space or hold meetings virtually.
With the upcoming holiday season, it is imperative that we continue these practices. We are not only battling coronavirus, we are also now well into the flu season.
Right here, right now is the time to remain vigilant.
More information about our plan for distributing the vaccine will be coming shortly. The COVID Vaccine Task Force will continue to manage the communication, distribution, and administration of the vaccine, which will be done in a manner that is safe, fair and equitable.
I want to thank our COVID Vaccine Task Force and Operations Command for their diligent and tireless work on this initiative. They have effectively worked together to reduce the negative impact on our people, patients and community since the onset of the pandemic several months ago. Please join me in thanking the members of the Task Force and Operations Command listed below for their efforts:
Thank you for everything you have done throughout this pandemic. I have never been prouder to work alongside each and every one of you.

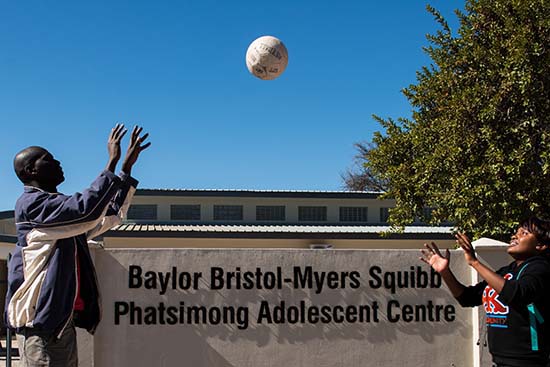
Texas Children’s, in partnership with Baylor College of Medicine, is saving the lives of children and women across the globe.
A network of physicians, fellows and residents provide much-needed clinical support as well as training and academic leadership to underserved communities in 18 nations in Africa, Romania, Papua New Guinea and Latin America. These global efforts began in 1999 with the creation of the Baylor College of Medicine International Pediatric AIDS Initiative at Texas Children’s Hospital, also known as BIPAI.
Under the initiative, the first Children’s Clinical Center of Excellence opened its doors in Constanta, Romania. Today, there are 14 such centers and satellite centers in eight countries across the world. The care provided at these centers has saved a generation of young people with HIV/AIDS and has given BIPAI a model from which to expand its services to both children and women.
The series of stories you will see on Connect over the next few months will talk about why Texas Children’s started a global health program and why it is so important for us to maintain it, grow it and continue to support it.
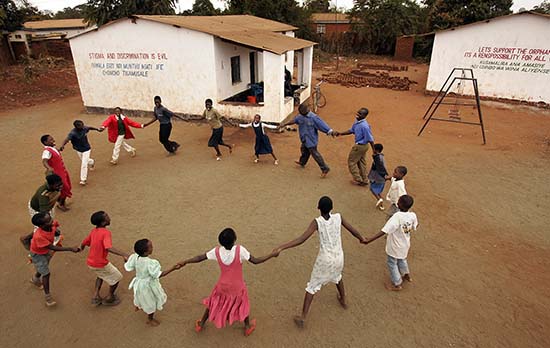
The series will highlight our efforts in Malawi because members of the Corporate Communications team traveled there last summer to gather stories, video and photographs in order to better educate our internal and external audiences about our efforts overseas.
Since then, the COVID-19 pandemic has stopped travel to these areas and many of the others we serve, but Texas Children’s remains dedicated to our global health efforts and still has many clinicians on the ground across the globe. We are moving forward with capital projects that were in the works prior to the pandemic and are offering support services in any and all ways possible both to help the people in these countries overcome the pandemic and to maintain the progress that’s been made in these areas over the past 20 years.
“It’s imperative we protect the gains we’ve made,” said Michael Mizwa, chief executive officer of BIPAI. “COVID-19 has the potential to wipe out years of work in areas where we are seeing significant gains. We cannot give up on the children and women in these countries now. They need us more than ever.”
Tune in next week to learn more about when, where and how Texas Children’s global health initiatives began and why they are making such a positive impact on the children and women they serve.














The US Constitution, Article 1, Section 2, mandates that every ten years, the country must conduct a count of its population. Today, that count is done by the non-partisan, US Census Bureau for every state and our five US Territories.
Besides knowing how many people live in the United States and our territories, the census informs elected officials, health authorities, school boards, and civic leaders about the communities they serve and the needs of its residents. The 2020 Census will determine how over $800 billion in federal tax dollars gets allocated and apportions how many elected representatives we have in Congress and creates new districts for future office holders. The Census helps state and local leaders decide where schools and health clinics are built, what infrastructure and transportation projects should be prioritized, and informs us of the composition of US households across our great country. For these reasons and others, it is critically important that we all respond to this year’s census.
The average census response rate for the US is 88 percent, but as of early September 2020, Texas is behind this average at 85 percent. This lower response rate means Texas could forgo crucial funding and resources which could then be redirected to other states with a higher response rate.
Every member of our One Amazing Team should perform this civic duty and respond to the 2020 Census questionnaire before the September 30 deadline. We urge you to encourage your family and friends to do the same.
There are four easy ways to respond to the Census and it only takes two minutes to complete!
Secure Internet: For the first time this year, the Census will be available online.
https://2020census.gov/en/ways-to-respond/responding-online.html
Respond by phone: The census phone lines are available at 1-800-923-8282.
https://2020census.gov/en/ways-to-respond/responding-by-phone.html
A significant undercount would dramatically deprive our region of vital public and private resources for the next ten years! Go to https://www.2020census.gov now and get counted!
This week on Mark Wallace’s blog, he takes a look at how the pandemic has inspired all forms of leadership. Read more

Like most parents, the Harts were nervous about their 10-month-old son’s surgery scheduled with Texas Children’s Division of Urology. In addition to regular jitters, they were especially concerned about their son undergoing general anesthesia.
“My husband did some research and found that it can be dangerous for young children,” Kayla Hart said. “So, needless to say, we were a little worried.”
Those worries were put to ease when their son’s pediatric anesthesiologist, Dr. Kevin Chu, and surgeon Dr. David Roth, explained the information the couple found online and offered another option, spinal anesthesia. Spinal anesthesia, numbs the lower part of the body to block pain versus general anesthesia, which puts a patient to sleep.
Texas Children’s Department of Anesthesiology and Department of Surgery recently started offering spinal anesthesia, when appropriate, to parents of young children. Rowan Hart was one of the hospital’s first patients to receive spinal anesthesia as an alternative to general anesthesia.
“When I went back to recovery, he woke up from the nap he was taking throughout surgery and was totally normal,” Hart said. “He wasn’t groggy at all and was even smiling.”
General Anesthesia Division Chief Dr. Olutoyin Olutoye said spinal anesthesia is a safe alternative to general anesthesia in patients under one year of age who are having surgery on the lower part of their body. She said if needed, the patient may receive a light sedative to make them relax but otherwise, they are awake during their procedure. There is no need for a breathing tube when a child receives spinal anesthesia and patients, like Rowan Hart, are alert and in good spirits post operatively.
“Even though anesthesia is much safer today than ever before, every anesthetic exposure and surgical encounter, has an element of risk and we must remain vigilant about communicating such risks to our patients and their families,” Olutoye said. “Offering an alternative to general anesthesia when appropriate is another way we can serve our patients and families in this capacity.”
On December 14, 2017, the U.S. Food and Drug Administration (FDA) released a drug safety communication about prolonged or repeated anesthetics in young children and pregnant women in their third trimester.
The FDA’s communication states:
As a result of the communication Texas Children’s Hospital changed its anesthesia practice and started discussing the warning before surgery with the parents of all children 3 years of age and younger.
In addition, Texas Children’s Hospital adopted the warning’s recommendation that a discussion occur among parents, surgeons, other physicians and anesthesiologists about the duration of anesthesia, any plan for multiple general anesthetics for multiple procedures, and the possibility that the procedure could be delayed until after 3 years of age. Parent-education materials that cover these topics are available to our patients and their families.
“I think offering spinal anesthesia is another way we can remain on the leading edge of this issue,” said Roth, who helped spearhead the use of spinal anesthesia together with the Department of Anesthesiology, and who has operated on the patients who have received it thus far. “It’s a safe alternative that we can use to reduce any potential risks of general anesthesia in our younger population.”
Anesthesiologist-in-Chief Dr. Dean B. Andropoulos agreed and said the benefits of anesthesia must always be weighed against the risks of anesthesia itself and Texas Children’s does a good job at doing that.
“We are very serious about educating our patients and families prior to surgery about any risks and any options that can be taken to mitigate such risks,” Andropoulos said. “Using spinal anesthesia is a nice addition to what we already are doing to mitigate potential risk.”

We can do just about anything these days with our smartphones. We can send and receive emails, make online purchases, connect with family and friends on social media, schedule doctors appointments and even access our medical health records, thanks to smartphones and modern software applications.
In our IT driven world, patient and provider communication should be conducted quickly, securely and conveniently, especially when it comes to accessing and exchanging electronic health information.
In 2016, The Office of the National Coordinator (ONC) for Health Information Technology passed federal legislation called the 21st Century Cures Act Final Rule that puts patients in charge of their health care by allowing them to access their electronic health information more easily through the use of smart phone applications of their choice. The interoperability, information blocking, and patient access to data and electronic health record certification requirements outlined in the 21st Century Cures Act will go into effect in multiple phases and will impact our patients, health care providers and health IT software developers.
The Information Blocking provision under the 21st Century Cures Act is the first phase that will go into effect on November 1, and will impact access, exchange or use of electronic health information. The Information Blocking rule will apply to patient portals and applications – like MyChart, Care Everywhere and EpicCare Link – where a patient can easily access their medical records online. However, the rule does not apply to Texas Children’s traditional medical record information release process, where a patient has to go through the Medical Records Office to request copies of their personal health information.
Some of the core data elements that will require autorelease through our patient portals include allergies, assessment and plan of treatment, clinical notes, clinical care teams, health concerns, immunizations, lab results, medication, demographics, procedures, unique device identifiers for implants, and vitals data.
“Under the new rule, health care providers could be liable for information blocking if they do not release this data through these patient portals,” said Brian Stanford, Director of Health Information Management. “Right now, most of this data is not automatically released. Starting in November, we will be required to release this data via MyChart and other patient portals to make it more accessible so patients don’t have to go through the traditional medical record release process to obtain a copy of their health information.”
While there are a few exceptions to the information blocking rule – for instance, psychotherapy clinical notes are exempt from being automatically released into a patient’s electronic health record – this new process of information sharing will be a culture change for our health care providers and our patients.
“Our providers are used to reviewing health reports first before contacting their patient to discuss the results and plan of care,” said Maggie Weimer, Practice Administrator for Transition Medicine. “Now that this health information will be released automatically into the patient portal, a patient could access this information before their provider has had the chance to reach out to them to discuss their results. This change can come as a shock to the patient, especially if there is a particularly sensitive diagnosis.”
To prepare and educate the organization about the Cures Act, a workgroup has been assembled to carefully review the regulation, review our policies, procedures and business practices, and develop a systemwide communication plan to ensure our providers are compliant with this new federal regulation.
“With regard to information blocking exceptions, we are working with our legal department to carefully review certain situations where we could block the autorelease of information if the provider feels that releasing this information could potentially cause reasonable harm to the patient,” said Stanford. “We are collaborating with our IS team, senior executive leadership, and our MyChart and patient information exchange workgroups to help us evaluate and determine what our obligations are around the Cures Act.”
In addition to the ONC Final Rule, The Center for Medicare and Medicaid Services (CMS) Final Rule includes additional requirements primarily for payers, that are also intended to increase interoperability.
“As more provisions go into effect in the upcoming year, our Cures Act workgroup team will continue to meet regularly to ensure the organization is informed, prepared and compliant,” said Weimer. “We are working with our internal partners and Marketing to help us facilitate timely communications as needed.”
Stay tuned to Connect for more updates on the Cures Act and the organization’s implementation efforts.