The following is based on information from a story published in TMC and a series of interviews conducted with Dr. Daniel Penny, chief of pediatric cardiology, Dr. Eyal Muscal, chief of rheumatology, and Dr. Lara Shekerdemian, chief of critical care.
In recent weeks, health experts in the United States and abroad began to notice a troubling rise in multisystem inflammatory syndrome in children (MIS-C), a condition in which various organs — such as the heart, lungs, kidneys, brain, skin, eyes, esophagus, stomach and intestines — become inflamed. Earlier this month, the Centers for Disease Control and Prevention (CDC) issued a health advisory to warn doctors about the illness, cautioning them to be on the lookout for a constellation of symptoms, including fever, abdominal pain, vomiting, diarrhea, neck pain, rash, bloodshot eyes and lethargy.
Although the exact cause of MIS-C is still unknown, experts are assessing the association between MIS-C and COVID-19, as many children diagnosed with the syndrome have been infected by or previously exposed to SARS-CoV-2, the virus that causes COVID-19.
This lag between the primary infection and the inflammatory response is what is interesting,” Penny said. “What it appears to indicate is that this is not a manifestation of the primary infection with SARS-CoV-2 itself, but rather the body’s inflammatory response to the infection.”
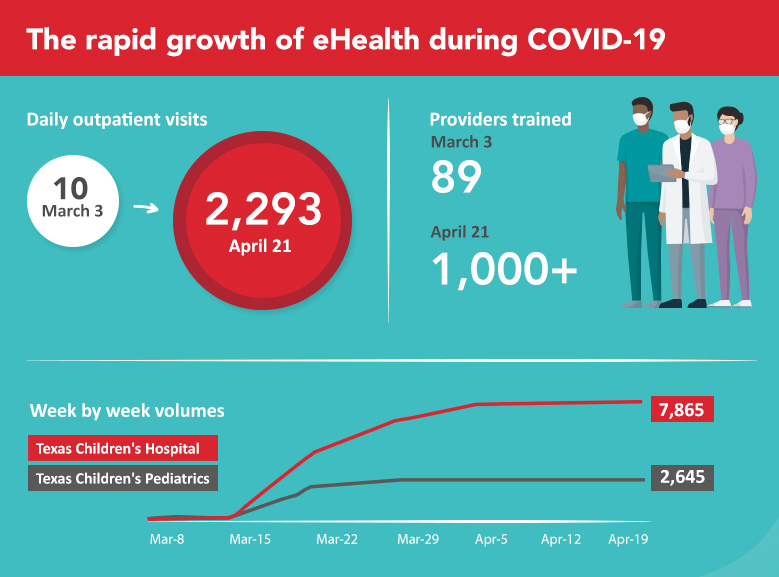
Texas Children’s is treating children and young adults with the syndrome and Penny is leading a cardiology clinic dedicated to those who have previously had SARS-CoV-2 infection in order to make sure that the handful of patients the hospital has already treated is not just the tip of the iceberg.
“Even if they weren’t extremely unwell in the first place,” he added, “we are bringing back these children for cardiology assessment with a cardiography in order to make sure they don’t have abnormalities of the coronary arteries that haven’t manifested clinically at this stage but could be problematic in the longer term.”
Not all children with MIS-C exhibit the same symptoms, the CDC noted, but doctors and parents should be vigilant of emergency warning signs, such as trouble breathing, persistent pain or pressure in the chest, new confusion, inability to wake or stay awake, bluish lips or face and severe abdominal pain.
Symptoms associated with MIS-C were first reported by clinicians in the United Kingdom in late April and have since been identified in other European countries and the United States, starting in New York, the American epicenter of the coronavirus outbreak. At least 17 other states have reported cases of MIS-C, including Texas, California and Washington.
Doctors believe that MIS-C is caused by an overactive immune system in response to COVID-19, leading to abnormal inflammation throughout the body. Most children recover from MIS-C after being treated with immunoglobulins to reset the immune system, steroids and immunosuppressive drugs, such as anakinra and tocilizumab; however, in rare cases, the illness can lead to death.
Understandably, this is very worrying to parents and Texas Children’s has received many questions and concerns about MIS-C. The following are some of those questions and our answers. We are sharing them with our employees because many of you are parents yourselves and might have some of the same concerns.
What are the early signs and symptoms of MIS-C and is there anything parents should be looking out for during the early stages of this condition?
Dr. Muscal: Based on experiences in Europe and the East Coast, so the places in the world that have had a head start on us here in terms of the multi-system inflammatory type of syndrome, it appears as if kids often have unrelenting fever that doesn’t really respond to traditional anti-inflammatory measures. And then, usually, a variety of other problems such as abdominal pain, vomiting, inability to keep fluids down, and then usually a variety of issues like rash, sometimes red eyes, and a general appearance of ill appearance. It appears that those are some of their early symptoms. As a child’s become more ill, perhaps he or she will have chest pain or have more difficulty with their breathing.
How common is MIS-C in children, how long does it last and how serious can it actually get?
Dr. Muscal: It appears that MIS-C is pretty uncommon, actually rare, according to some of the other cities that have had cases for a longer period. Some of the experts in New York city believe that less than 1% of the children that actually are exposed to the coronavirus and get COVID-19 seem to develop this more serious post-infectious process. It can last for days or even a couple of weeks as kids recover from it. It appears to be in many cities with more cases, that most of the cases are treated quickly and are not that serious. Though there are kids that end up in the intensive care unit and unfortunately, exceptionally rare, kids that pass away.
What ages are most typically affected, and how old are the oldest children who do get MIS-C?
Dr. Muscal: So again, with the last six weeks of knowing more about this condition, it appears that even if children have some of the features of another entity called Kawasaki disease, they appear to be a little bit older. So perhaps even teenagers that are getting this, whereas Kawasaki disease is usually a disease of early childhood. It does appear that perhaps young adults can also have features of this syndrome. Unfortunately, many adult physicians have never seen Kawasaki disease and it could be that they’re not aware of some of these signs and symptoms.
Does it seem to be that children with underlying illnesses are more prone to get MIS-C?
Dr. Penny: We don’t believe that this condition is more common in children with preexisting conditions. So what it seems to be is that a child gets the coronavirus infection, and then they get this overactive immune response to the infection. And that’s what results in this syndrome. And so this does not appear to be more common in children who have underlying diseases, such as congenital heart disease.
If a child has congenital heart disease, let’s say a relatively simple defect like an ASD or even something more complex, are they going to be at higher risk of getting MIS-C?
Dr. Penny: We haven’t seen any patients with congenital heart disease who’ve developed MIS-C in our hospital, and I think it’s quite rare throughout the world. I don’t see any reason to believe why children with congenital heart disease will be at more risk of developing the syndrome in the first place. And also, if you have well compensated heart disease, I also don’t believe there should be any particular risk to a patient if they did happen to get the condition in the setting of congenital heart disease.
What is the difference between MIS-C and Kawasaki disease? And does this new syndrome seem to only affect kids who have COVID-19?
Dr. Penny: So MIS-C refers to this syndrome that we see in children, particularly related to coronavirus infection. And that’s according to the recent CDC definition, and this is really specific to coronavirus infection. But we do see similar conditions in other situations. What we see in patients with Kawasaki disease is that, that they get dilated coronary arteries. These abnormal coronary arteries are also seen in some patients with MIS-C. Typically, though, it doesn’t seem to be as common in MIS-C as in Kawasaki disease. One of the other differences between MIS-C and Kawasaki disease is Kawasaki disease tends to be clustered in much younger children. Whereas MIS-C, as we said earlier, can affect older children and even adults.
How many cases of the syndrome do you think we’ve had in Houston so far? And do you expect these cases to rise as they have in other cities on the East Coast?
Dr. Shekerdemian: We have seen a handful of patients with MIS-C at Texas Children’s. We don’t have an exact number because we obviously investigate many more than we end up diagnosing according to the strict criteria. It would certainly be less than 10. And the question about expecting them to rise, it’s a difficult one to answer. I think what we’re seeing in terms of the density of MIS-C around the world, not just in the US, very much mirrors the density of primary COVID-19 infection in those cities. So luckily Houston was not hit anything like as badly or hard in terms of severe COVID-19 infection. I think that would really speak to the fact that, while we’re seeing patients present with MIS-C, it seems to be a steady number. We’re not seeing a huge explosion and, touch wood, we hope that’s going to continue.
Do you think patients who have MIS-C, in general, are they still contagious with coronavirus?
Dr. Shekerdemian: That’s a really important question. We believe that the majority of them will not be contagious at the time that they develop the MIS-C. The typical presentation is around the four week mark, after a primary COVID-19 infection. And the vast majority of children at that stage, or anybody contracting COVID-19, would likely be non-contagious. Of course, we do test them with nasal swabs, as well as the typical antibody tests that are required to confirm the diagnosis. So I think it’s reassuring to a point that most children are not contagious, but we do screen them just in case they’ve still got signs of any active COVID-19 disease.
Is it safe to send children back to daycare or school once they reopen?
Dr. Shekerdemian: To be perfectly honest, there isn’t a simple answer to that. As COVID-19 stays in the community, we have to be hyper vigilant. What I would want to know before sending a child or a loved one to a school or daycare or summer camp is, what sort of screening; the numbers of children or adolescents in a specific space; the respect for social distancing, for hygiene, for hand-washing, etc. and how they’re going to screen any care takers or any workers in those environments, I would hope, on a daily basis; and feedback constantly to parents and to caregivers to reassure them and provide constant updates.