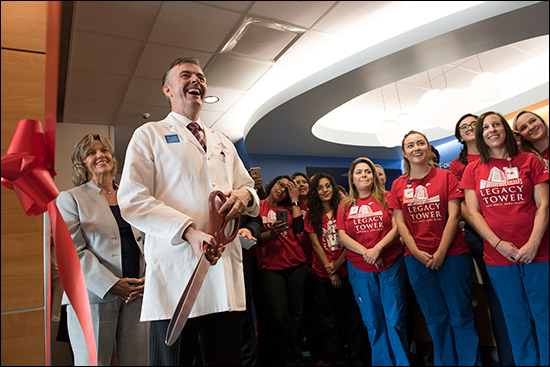
Early on the morning of November 7, an excited group including Texas Children’s Hospital clinical leadership, executives and members of the Kangaroo Crew and Mission Control teams gathered on the roof of Lester and Sue Smith Legacy Tower for a special ribbon cutting ceremony marking the opening of our new helistop.
Watch the video or view the photo gallery below.

“The Lester and Sue Smith Legacy Tower has always been about improving care for the sickest children we see,” said Surgeon-in-Chief Dr. Larry Hollier. “The helistop is important because it improves access for those children. Whether they’re being transported as part of a scene response for an auto accident or transferred from another hospital, we can now get children and women here in very rapid fashion within a 150-mile radius.”
The helistop is the final element of Smith Legacy Tower to go live and represents the culmination of a major expansion at our Texas Medical Center campus. Months of planning and multidisciplinary cooperation between medical staff, Transport Services and engineering and facilities teams went into preparations for the helistop opening.
“A tremendous amount of work has gone into making sure that the helistop is very safe – safe for the helicopters coming in, safe for those crew that are delivering the patients to us, and safe for our own staff,” said Executive Vice President Mark Mullarkey. “Bert Gumeringer, Gail Parazynski and Deb D’Ambrosio and their teams have been instrumental both in making sure we’re prepared to open the helistop and really in bringing Smith Legacy Tower to full completion.”
Extensive simulation exercises were also held to prepare care and transport teams for potential eventualities they may face, as well as to analyze and improve processes. This included helicopter landings, transferring patients from the helicopter crew to Texas Children’s transport teams, and moving patients from the helistop at Smith Legacy Tower to Trauma and the Emergency Center.
“The helicopter simulation was fantastic,” said Dr. Jeanine Graf, chief medical officer at West Campus and pediatric medical director of the Kangaroo Crew. “We brought together members from our trauma, surgery, ICU and NICU teams, as well as our experts in maternal-fetal medicine, for training and simulations, which were coordinated by our Texas Children’s Simulations Center. Dr. Cara Doughty really did an excellent job demonstrating how more than a hundred folks would be involved in the communication and execution of a helicopter landing at Texas Children’s.”
The helistop at Smith Legacy Tower is the third helistop in the Texas Children’s system, with others in operation at West Campus and Texas Children’s Hospital The Woodlands. The addition of the new helistop will facilitate the rapid transport of patients across all populations, including neonatal and maternal patients. Before the helistop opening, Texas Children’s received roughly 150 helicopter transports a year, which landed at nearby partner institutions. Now with our own helistop, we’ll be able to offer our care to even more patients who need us.
“The helistop really changes things for us,” said Deb D’Ambrosio, RN, director of Transport Services and Mission Control. “We’re certainly expecting high volume, but with the processes we’ve developed with our helicopter vendors and the high level of coordination between Transport Services and Mission Control, this is going to be so much better for our patients.”















 As the largest children’s hospital in one of the fastest growing cities in the country, Texas Children’s high-quality care is always in high demand. However, due to high volume, getting patients and referring providers the answers and access they need in a timely fashion can be a challenge, which is why improving access has been a key focus at Texas Children’s in recent months.
As the largest children’s hospital in one of the fastest growing cities in the country, Texas Children’s high-quality care is always in high demand. However, due to high volume, getting patients and referring providers the answers and access they need in a timely fashion can be a challenge, which is why improving access has been a key focus at Texas Children’s in recent months.














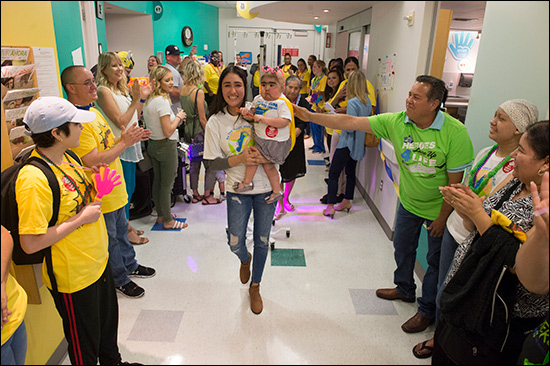
 As part of National Childhood Cancer Awareness Month, Texas Children’s Bone Marrow Transplant Unit (BMT) was transformed for a few hours last week into a full-fledged parade route – music, costumes and all.
As part of National Childhood Cancer Awareness Month, Texas Children’s Bone Marrow Transplant Unit (BMT) was transformed for a few hours last week into a full-fledged parade route – music, costumes and all.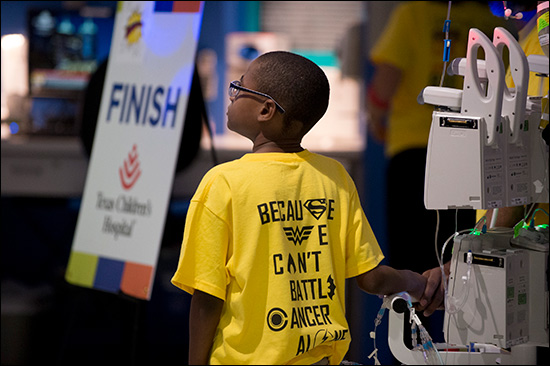
















 Imagine you’re the parent of a newborn with an arm injury. During your admission you’re told not to move the arm and to protect it all times. Now imagine coming back for your clinic appointment and hearing that it’s time to start moving the arm at home – unsupervised. For parents of children with brachial plexus birth palsy, this moment can be daunting.
Imagine you’re the parent of a newborn with an arm injury. During your admission you’re told not to move the arm and to protect it all times. Now imagine coming back for your clinic appointment and hearing that it’s time to start moving the arm at home – unsupervised. For parents of children with brachial plexus birth palsy, this moment can be daunting.