Texas Children’s Hospital’s Trauma Center has received the prestigious 2018 Trauma System of Care Award from the Southeast Texas Regional Advisory Council (SETRAC). The Trauma System of Care Award recognizes Texas Children’s Hospital as one of the best in SETRAC’s nine-county region for excellence in the development and advancement of pediatric trauma services.
At a recent awards ceremony, SETRAC honored Texas Children’s as well as other hospitals and first responders who have exhibited outstanding performance in areas such as trauma care, stroke care, cardiac care, multi-agency teamwork, disaster preparedness and citizen hero of the year. The ceremony was held at the Hilton of America’s and was attended by nearly 700 individuals and elected officials, including State Representatives, City of Houston EMS Physician Director Dr. David Persse, and Jim “Mattress Mack” McIngvale, owner and operator of Gallery Furniture.
“This award means a lot because, being only in our eighth year, we are the youngest Level I trauma center in Houston,” said Dr. Bindi Naik-Mathuria, Trauma Center director. “We have come a long way in developing programs to provide the best care for injured children as well as injury prevention education for our community. It was rewarding to be recognized as the best pediatric trauma hospital in the region.”
Texas Children’s Hospital has been verified as a level I Pediatric Trauma Center since 2010. The level of verification was requested by the hospital and the on-site review of the hospital was conducted by a team of reviewers experienced in the field of trauma. Using the current Resources for Optimal Care of the Injured Patient manual as a guideline, this team determined if the criteria for the requested level have been met.
Established by the American College of Surgeons in 1987, the Consultation/Verification Program for Hospitals promotes the development of trauma centers in which participants provide not only the hospital resources necessary for trauma care, but also the entire spectrum of care to address the needs of all injured patients. This spectrum encompasses the prehospital phase through the rehabilitation process. Verified trauma centers must meet the essential criteria that ensure trauma care capability and institutional performance.
SETRAC was founded by the late Dr. James H. “Red” Duke, Jr., legendary trauma surgeon at Memorial Hermann-Texas Medical Center and John B. Holmes Professor of Clinical Sciences at UT Health Medical School, and has been funded by the Texas Department of State Health Services for the last 25 years.
April 10, 2018
After two independent studies were published two years ago suggesting that the maternal mortality ratio (MMR) in Texas had doubled within the past decade, an updated report released today in the journal Obstetrics & Gynecology found that the MMR in Texas was significantly lower in 2012 than previously reported due to data collection error. The identification of this error illustrates an important role of the maternal mortality review process – ensuring accurate data on which to base interventions.
Comprised of 15 Texas-based multidisciplinary experts and chaired by Dr. Lisa Hollier, chief medical officer at Texas Children’s Health Plan and professor of obstetrics and gynecology at Baylor College of Medicine, the Maternal Mortality and Morbidity Review Task Force used an enhanced methodology that combined data matching and records review for identifying maternal deaths. After meticulously reviewing 2012 data, investigators determined that the MMR in Texas was 14 to 18 deaths per 100,000 versus the 37 deaths per 100,000 previously reported.
“Our analysis found there were data quality issues,” said Hollier, who also is president-elect of the American College of Obstetricians and Gynecologists. “When we examined the data, it showed that some deaths were mistakenly coded as “dying while pregnant,” when there was never a pregnancy. Beginning in 2010, Texas transitioned from paper to electronic death certificates, so unintentional user error in reporting pregnancy status may be responsible for the inaccurate data.”
Texas’ current electronic death registration system displays pregnancy status options as a dropdown list. The “pregnant at time of death” option is directly below the “not pregnant within past year” option. The investigators concluded that this could have led to erroneous selection, and could explain why pregnancy at time of death was reported for nearly 76 percent of the 74 obstetric-coded deaths with no evidence of pregnancy upon review.
The task force determined that a total of 56 Texas resident maternal deaths occurred during pregnancy or within 42 days postpartum in 2012. The most common causes for these deaths were drug overdose and cardiac events.
While the MMR is lower than initially reported, the updated report confirms a vast disparity still exists – black women had a higher MMR (27.8 per 100,000 live births) than did women of other racial and ethnic groups. Black women in Texas have more than double the risk of dying during pregnancy or within 42 days postpartum.
As one of the nation’s premier facilities for women’s, fetal and newborn health, Texas Children’s Pavilion for Women remains actively involved in grassroots advocacy at state and national levels with the goal of improving health outcomes, quality of care and patient safety for women and newborns across Texas and the nation.
Through the efforts of the Maternal Mortality and Morbidity Review Task Force, Texas Children’s maternal-fetal medicine physician leadership is helping to review cases and study trends in maternal deaths so that we can better understand the problem and make recommendations to help reduce the MMR across Texas.
While these results published in the new report likely have national implications – since miscoding of obstetric deaths may occur in other states and affect the accuracy of their MMRs – the updated data demonstrates that Texas is more in the middle of the pack when it comes to MMRs across the nation.
“We believe future efforts should focus on improving the quality of death certificate data, especially pregnancy status,” Hollier said. “It is also critically important we don’t lose the unfortunate truth that even this updated data demonstrates a huge disparity between the MMRs faced by black women compared to women of other racial and ethnic groups. We need to continue work to identify why this disparity exists and create strategies to remedy it.”
Click here to read the report in the medical journal Obstetrics & Gynecology.
March 29, 2018
While the nation is glued to their TVs watching the NCAA’s “March Madness” college basketball tournament, Texas Children’s is focused on scoring patient access points during MyChart Madness.
On March 19, Texas Children’s launched MyChart Instant Activation and Fast Pass as part of the hospital’s system-wide initiative to improve patient access. MyChart is an online patient portal where patient families can schedule clinic appointments, communicate with their health care providers and access their health records at any time.
“When we implemented MyChart in 2010, one of our goals was to enable parents to become active participants in their child’s health care,” said Julie McGuire, director, Enterprise Systems Clinical, at Texas Children’s. “Through these recent enhancements to MyChart, we are continuing to cultivate a positive experience for our patients, children and women, and their families, while delivering the highest level of care possible.”
MyChart Instant Activation
MyChart Instant Activation essentially pushes out a text or email notification to Texas Children’s patient families that allows them to sign up for a MyChart account. Instead of having to use a computer to sign up, families who receive the invitation can now use a smart phone to activate their MyChart account and download the MyChart mobile app. Clinic staff at Texas Children’s Pediatrics (TCP) and Mark Wallace Tower have seized on the excitement of this new notification tool – and the current excitement around the college basketball tournament – by joining in a collaborative MyChart Madness competition. Other campuses like Texas Children’s Hospital West Campus have been successful in implementing MyChart Mondays where patients and their families can register on the spot.
“Our employees and staff have embraced this friendly and collaborative competition which has had a positive impact on patient access,” said Rachel Norman Brock, manager of Ambulatory Clinics at Texas Children’s. “Instant Activation provides the organization with another way to increase MyChart activation rates across the hospital system, resulting in more patients and their families taking advantage of the benefits of this online patient portal.”
The MyChart Madness teams are grouped in regions – Midwest, West, East and South – and the winner of the entire bracket receives a prize. MyChart Madness originated with TCP. TCP staff and employees launched the push to increase activations on March 1, and within just three weeks, the practices activated 9,003 new MyChart accounts. TCP’s success in promoting MyChart activations across its 51 practices inspired leaders across the organization.
During the first week of instant activation across the Texas Children’s hospital system, we had 3,492 same-day activations, almost half of which resulted from instant activation. This was a significant increase considering that a month ago, prior to the launch of MyChart instant activation, we had only 1,972 same-day activations.
Currently, several of our Texas Children’s Health Centers are doing an outstanding job of increasing MyChart activations. Cy-Fair Health Center achieved 100 percent same-day activations the week of March 11.
Fast Pass
Once families have activated a MyChart account, they have access to features like Fast Pass, which also recently launched with two subspecialties on March 19. Fast Pass creates an electronic waitlist, and automatically offers patients and their families on the waitlist sooner appointments. Patients also have the ability to add themselves to the waitlist via MyChart.
Just last week, a patient who had an April 12 appointment with Allergy/Immunology at the Sugar Land Health Center was seen 21 days sooner than originally scheduled when an opening became available at the Wallace Tower.
“Since Fast Pass went live, there have been seven Fast Pass offers accepted to help families get earlier appointments,” said Julie Barrett, director of Outpatient and Clinical Support Services at Texas Children’s. “We are so proud of our teams and their diligent work in helping us achieve these recent success stories on patient access.”
MyChart Instant Activation and Fast Pass are both tactics in Texas Children’s strategy to improve patient access. In just three short weeks since Texas Children’s launched the patient access initiative on March 1, the hospital has added 10,000 new patient appointments annually into the system. After evaluating appointment templates for over 200 providers, additional slots were found where physicians could see patients in four hour blocks.
“We must ensure that all patients have access to the amazing clinical programs offered at Texas Children’s,” said Texas Children’s Assistant Vice President Carrie Rys. “Our Patient Access Committee has identified many system-wide solutions that will enhance patient experience across the system. These will be implemented in phases over the next several months. Improving patient access at Texas Children’s is our focus and priority.”
March 6, 2018
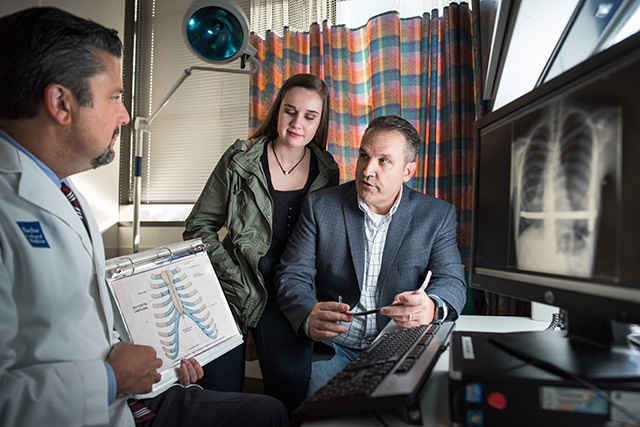
It’s not every day that physicians at Texas Children’s get the opportunity to treat a child and their parent, but that’s exactly what happened when Caitlin King became a patient of Texas Children’s Pectus Program.
The program is part of Texas Children’s Division of Pediatric Surgery and is run by a specialized team that assesses and treats an assortment of chest wall abnormalities such as pectus excavatum, where the chest has a sunken or caved-in appearance, and pectus carinatum, where the chest bows outward.
Caitlin King, 15, came to Texas Children’s in 2017 seeking help for pectus excavatum, a condition her father, Niky King, had suffered from since he was an early teen. Niky said he got his chest looked at when he was about 12 or 13, but doctors told him there was nothing wrong and that the issue was just cosmetic. When Caitlin was born, Niky said he hoped she would not inherit the same condition, but that if she did, doctors would be able and willing to do something about it.
“My chest affected my life dramatically,” said Niky, who used to have heart palpitations and difficulty taking deep breaths. “I was very self-conscience of it, and am convinced it hindered my ability to do physical activity for a sustained period of time.”
After assessing Catlin, Dr. Mark Mazziotti, a pediatric surgeon with the Pectus Program, assured the teenager and her father that he could correct her pectus excavatum via a minimally invasive surgery called the Nuss procedure. During this procedure, a curved stainless steel bar is inserted in the chest through small incisions on either side, and is guided between the sternum and the heart under direct visualization with a camera through a small incision in the right chest. The bar is left in place for about three years. Recurrence of the pectus excavatum after the bar is removed is very rare.
“This is a very rewarding procedure for the patient,” said Mazziotti, who surgically corrects about 50 pectus excavatum surgeries a year. “We have excellent outcomes, and Caitlin’s case has been no different.”
Since her surgery, Caitlin said “she’s been able to wear whatever she wants” because her chest already looks so much better. She also said she can exercise and maintain a normal, active lifestyle without any hesitation.
“I can’t tell the bar is there at all,” she said. “I’m very happy I decided to move forward with the procedure.”
Caitlin’s procedure went so well, Niky underwent the same procedure three months later. Mazziotti performed the procedure, and because of the severity of Niky’s pectus excavatum, inserted two bars instead of one. The results, Niky said, have been fantastic, just like his daughter’s.
Mazziotti attributes the great outcomes the Caitlin and Niky, and other pectus patients have had to the skill of the surgeons in the program and the fact that they have the ability to offer the most cutting edge technology and procedures. He also said the program’s partnership with anesthesiology and pain management is key as patients typically have to stay in the hospital for several days to recover.
“Texas Children’s Pectus Program is highly specialized and prides itself on offering individualized care,” he said. “We are privileged to be able to treat patients across Texas, the region and the country.”
For more information and to watch a video about our Pectus Program, click here.
February 13, 2018
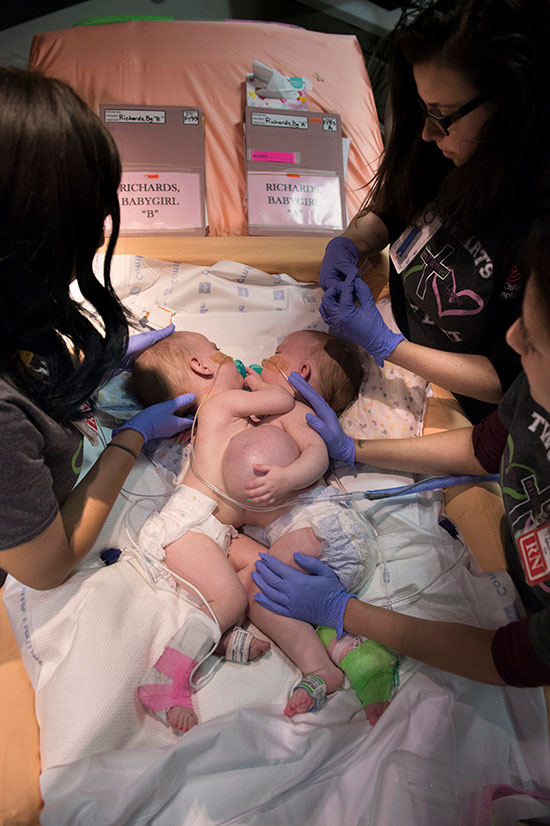
On January 13, Texas Children’s successfully performed its fourth conjoined twins separation, giving identical twin girls Anna Grace and Hope Elizabeth Richards a chance at a normal life.
The 7-hour procedure was performed by a multidisciplinary team of nearly 75 surgeons, anesthesiologists, cardiologists and nurses from eight specialties. Click here to see a list of surgeons, clinicians and nurses in the operating room during the milestone procedure, and here to view a photo gallery documenting the twins’ journey the day of their separation.
“The success of this incredibly complex surgery was the result of our dedicated team members’ hard work throughout the last year,” said Surgeon-in-Chief and Chief of Plastic Surgery Dr. Larry Hollier. “Through simulations and countless planning meetings, we were able to prepare for situations that could arise during the separation. We are thrilled with the outcome and look forward to continuing to care for Anna and Hope as they recover.”
The girls were born on December 29, 2016, at Texas Children’s Pavilion for Women to their parents Jill and Michael, and two older brothers Collin and Seth. Weighing a combined 9 lbs. 12 oz. and delivered via Caesarean-section at 35 weeks and five days gestation, Anna and Hope were conjoined at their chest and abdomen, through the length of their torso and shared the chest wall, pericardial sac (the lining of the heart), diaphragm and liver. In addition, they had a large blood vessel connecting their hearts.
The Richards family, from north Texas, learned Jill was carrying conjoined twins during a routine ultrasound. The family was then referred to Texas Children’s Fetal Center, where they underwent extensive prenatal imaging, multidisciplinary consultation and development of plans to achieve a safe delivery and postnatal care. They temporarily relocated to Houston in order to deliver at Texas Children’s and be close to the girls during their hospital stay. For the past year, Anna and Hope have been cared for by a team of specialists in the level IV and level II neonatal intensive care unit (NICU).
Planning and preparation
During much of that time, medical staff prepared for the separation, using extensive imaging with ultrasound, echocardiography, CAT scans, magnetic resonance (MRI) and even a virtual 3-D model of the girls’ anatomy. Closer to the surgery date, almost 50 medical personnel involved in the procedure participated in a lengthy simulation of the separation.
“These are the kind of procedures you plan for the worst and hope for the best,” said Pediatric Surgeon and Co-Director of Texas Children’s Fetal Center Dr. Oluyinka Olutoye. “We were blessed that this was the best case scenario. Everything went very well. The procedure was as well as we could have hoped.”
The Richards family is grateful to Texas Children’s for the care provided to their daughters since they found out they were expecting conjoined twins.
“We’ve thought about and prayed for this day for almost two years,” said the girls’ mom, Jill Richards. “It’s an indescribable feeling to look at our girls in two separate beds. We couldn’t be more thankful to the entire team at Texas Children’s for making this dream come true.”
Anna and Hope are recovering in the CVICU and expect to be released to a regular room soon. Both girls will face additional surgeries in the future to ensure their chest walls are stabilized. Otherwise, doctors expect them to lead normal lives.
“What we try to do here at Texas Children Hospital is essentially provide our patients with as normal of a life as we can,” said Pediatric Plastic Surgeon Dr. Edward Buchanan. “I think in this case with these two little girls we were able to achieve that.”
A history of success
The Richards separation is the fourth conjoined twins separation performed at Texas Children’s. The first pioneering procedure occurred February 16, 1965, when a team of surgeons separated 9-week-old conjoined twins Kimberly and Karen Webber. The Webber twins were connected at the liver and pericardium. The second separation happened on June 9, 1992, when Texas Children’s surgeons successfully separated Tiesha and Iesha Turner, who were 1 year old and shared a sternum, liver, entwined intestines and fused organs.
The third conjoined twins separation happened nearly three years ago on Feb. 17, 2015, when a team of more than 40 clinicians from seven specialties separated 10-month old Knatalye Hope and Adeline Faith Mata during a marathon 26-hour surgery. The twins were connected from the chest to the pelvis and shared a chest wall, pericardial sac, diaphragm, liver, intestinal tract, urinary system and reproductive organs. Today, Knatalye and Adeline are almost 4 years old and are doing very well, walking, talking, even learning how to ride a bike.
Since Texas Children’s opened its doors in 1954, multiple sets of conjoined twins have been referred to the hospital for consideration. However, in many of these cases, separation was not medically possible. Olutoye, who has participated in five conjoined twins’ separation surgeries, two at Texas Children’s Hospital and three at the Children’s Hospital of Philadelphia, said he and a team of experts from various specialties look at every case very closely and consider many factors before deciding how to move forward.
“Separating conjoined twins takes a tremendous commitment,” Olutoye said. “We all are privileged and honored to be part of each and every case, especially the ones where we can help.”
For nearly 17 years, Maryann Macey has volunteered with the Blue Bird Circle Clinic for Pediatric Neurology at Texas Children’s Hospital – an opportunity that she describes as very rewarding.
“It is amazing to see all of the progress our organization has made in advancing research to help our physicians at the Blue Bird Circle Clinic diagnose and treat patients with neurological diseases,” Macey said. “It is an honor to be a Blue Bird volunteer and work with such an outstanding group of women.”
On February 6, Macey and 100 Blue Bird members including many of Texas Children’s employees, staff and leaders, attended a special luncheon at the Pavilion for Women to celebrate the Blue Bird Circle’s 95th birthday. The event included a $1.9 million check presentation from the Blue Bird Circle to Texas Children’s and Baylor College of Medicine. A large portion of this gift will support neuroscience research and training.
Since 1998, the Blue Bird Circle has supported the Clinic for Pediatric Neurology at Texas Children’s with millions of dollars in grants, as well as thousands of volunteer hours. Blue Bird volunteers devote countless hours at the Clinic and The Blue Bird Circle Resale Shop which has helped to raise awareness in the community about pediatric neurological disorders and highlight the incredible work being done at Texas Children’s to improve the quality of life for neurology patients.
“The words, “Blue Bird Circle,” are synonymous with its members’ generosity, volunteerism, commitment and dedication,” said Texas Children’s CEO Mark A. Wallace. “Members of the Blue Bird Circle have been the catalyst for so much of what has happened in pediatric neurology in the past 20 years. The care we provide, the research we conduct because of the Blue Birds benefit the patients we serve here and children with neurological conditions all over the world.”
During the luncheon, Dr. Gary Clark, Chief of Neurology and Developmental Neuroscience, spoke about the tremendous growth of the neuroscience program at Texas Children’s and shared examples of the research progress that has been made through our partnership with the Blue Bird Circle. To treat patients with an enzyme deficiency in the form of Batten disease, Texas Children’s is one of the few sites that provides therapy to these patients by surgically injecting the synthesized enzyme directly into the brain thereby halting this degenerative form of Batten disease. Texas Children’s also is using novel approaches to treat patients with spinal muscular atrophy, a disease of the nervous system where the spinal cord degenerates due to defects in the SMN1 gene. The treatment involves injecting a DNA molecule into the spinal fluid that turns latent gene into an effective one that makes the deficient protein.
“We are contemplating similar treatments for Angelman and Rhett syndromes,” Clark said. “We are so grateful to Texas Children’s Blue Bird Circle Research Center in collaboration with the Jan and Dan Duncan Neurological Research Institute at Texas Children’s for helping us make these research breakthroughs possible, and I am excited about what the future holds for pediatric neurology.”
Guest speakers at the event also included Dr. Charles Gay, medical director of Neurology at Texas Children’s Hospital West Campus, and Dr. Robert Zeller, medical director of the Blue Bird Circle Clinic for Pediatric Neurology. Texas Children’s Chief of Palliative Care Dr. Tammy Kang delivered the keynote address on the interdisciplinary palliative care program and how it supports patients and their families.
Prior to the luncheon, the Blue Bird members met with neurosurgeon Dr. Daniel Curry and Chief of Critical Care Dr. Lara Shekerdemian to tour different sections of the Legacy Tower which will open on May 22.
For more information about Blue Bird Circle, click here.
Transplant teams with Texas Children’s Hospital performed 112 solid organ transplants in 2017, the most in the history of Texas Children’s Transplant Services.
The liver and the kidney transplant programs were the busiest with 42 liver transplants and 32 kidney transplants completed last year. The heart program completed 28 transplants in 2017 and the lung program finished with 10, including one transplant in a patient under the age of one. There were only three such transplants in the United States last year.
“I’m very proud to be working with a team so dedicated to providing the best possible outcomes for our patients,” said Dr. John Goss, medical director of Transplant Services. “This milestone demonstrates that Texas Children’s continues to earn its reputation as one of the best pediatric transplant programs in the country, and is a testament to the skill and commitment of our multidisciplinary team.”
Since its inception, Texas Children’s Transplant Services has grown at a steady pace and is now one of the largest pediatric transplant programs in the nation. Along the way, the transplant teams have hit many milestones: performing 98 solid organ transplants in 2014, completing four kidney transplants over the course of 18 hours in 2016, and in 2017, performing 112 transplants, a record number for the team, boosting its total number of transplants to more than 1,500.
One of the recipients of last year’s 112 transplants was 4-month-old Carter Kraft. Born on June 10, 2017, at a hospital in his home state of Florida, Carter immediately cried loudly, but nurses noticed fluid on his lungs. After a nerve-racking few weeks waiting for answers as to what was causing breathing issues for their son, Carter’s parents, Jennifer and Matt Kraft, were told their son had a rare genetic disorder called ABCA3 Surfactant Protein Deficiency, which prevented his lungs from being able to absorb oxygen. The only treatment for the disorder is a double lung transplant.
Carter was transferred to Texas Children’s Hospital on August 16 because our transplant teams have the depth of skill and unique qualifications to treat patients from newborns to young adults in need of a heart, kidney, liver and lung transplant. In particular, the hospital’s Lung Transplant Program offers a median wait time of less than four months and is one of only two institutions performing 10 or more pediatric lung transplants each year.
Carter spent time in the Neonatal Intensive Care Unit (NICU) before undergoing a procedure to repair a patent ductus arteriosus (PDA) of his heart. Then, on October 27, Carter underwent the double lung transplant he needed with Dr. Jeff Heinle, interim chief of congenital heart surgery at Texas Children’s.
Now, 12 weeks post-transplant, Carter is doing well and his family is looking forward to returning home to Florida soon.
“We are so pleased that we were able to help Carter and that he is doing so well,” Heinle said. “We are fortunate to work at Texas Children’s Hospital where we have the resources to provide this kind of specialized care to complex, challenging patients.”
For more information on Texas Children’s Transplant Services, click here. To watch a story on KHOU-TV Channel 11’s about Texas Children’s Transplant Services milestone, click here.
 Texas Children’s Hospital’s Trauma Center has received the prestigious 2018 Trauma System of Care Award from the Southeast Texas Regional Advisory Council (SETRAC). The Trauma System of Care Award recognizes Texas Children’s Hospital as one of the best in SETRAC’s nine-county region for excellence in the development and advancement of pediatric trauma services.
Texas Children’s Hospital’s Trauma Center has received the prestigious 2018 Trauma System of Care Award from the Southeast Texas Regional Advisory Council (SETRAC). The Trauma System of Care Award recognizes Texas Children’s Hospital as one of the best in SETRAC’s nine-county region for excellence in the development and advancement of pediatric trauma services.

 It’s not every day that physicians at Texas Children’s get the opportunity to treat a child and their parent, but that’s exactly what happened when Caitlin King became a patient of Texas Children’s Pectus Program.
It’s not every day that physicians at Texas Children’s get the opportunity to treat a child and their parent, but that’s exactly what happened when Caitlin King became a patient of Texas Children’s Pectus Program.




















 For nearly 17 years, Maryann Macey has volunteered with the Blue Bird Circle Clinic for Pediatric Neurology at Texas Children’s Hospital – an opportunity that she describes as very rewarding.
For nearly 17 years, Maryann Macey has volunteered with the Blue Bird Circle Clinic for Pediatric Neurology at Texas Children’s Hospital – an opportunity that she describes as very rewarding.