September 25, 2018

For months, teams have been preparing for the opening of the new Texas Children’s Heart Center® in Legacy Tower. The outpatient clinic went live on September 18. And this week, Move Day into our inpatient space has finally arrived.
Before the flurry of activity, we had the opportunity to sit down with new Chief of Congenital Heart Surgery Dr. Christopher Caldarone, who shared a little about his background and his vision for the No. 1 heart center in the nation.
Tell us a little about yourself. Where’d you grow up?
“I was born in Boston and grew up in Upstate New York and New Jersey. We still have a lot of family in Boston and spend time there in the summer.”
Were you always interested in medicine as a career?
“I had a predisposition toward engineering and science as a kid. I ruptured my spleen in a high school wrestling match and spent a few months in hospitals. I was fascinated by the environment and I think that’s when it really started for me. I went to college at Johns Hopkins for bioengineering but found the subject matter to be too dry. I realized I really liked the medical part of my studies, so I switched over to pre-med.”
How did that lead to your interest in surgery?
“Sometimes people find that they just fit in a field. You just feel like there are places in life where you belong and others you don’t, and I always felt like I belonged in surgery.”
How does it feel to be a part of the team at Texas Children’s?
“It feels amazing. I think that for those of us who’ve been at other institutions, it’s easy to appreciate how special this place is. It’s a spectacular environment.”
What was it about Texas Children’s that attracted you?
“It was all about fit and impact. I spent fifteen years in Toronto with a great team. But from the very first call from Texas Children’s, I felt that we shared a common vision and I felt that I was a good fit for what they were looking for in a very genuine way. That was very compelling. Secondly, the potential here to make a difference is vast. There is an opportunity to take what I learned in my previous role as surgeon-in-chief and refocus on congenital heart disease, which is the area that interests me the most.”
Why is multidisciplinary collaboration so important?
“Being part of a team and functioning as a team is my preferred environment. I just enjoy it more. But that isn’t the reason why it’s important. It’s important because the congenital heart program at Texas Children’s is already competing at the Olympic level. The gradations between the best pediatric hospitals are so fine that to compete at this level, you have to optimize every aspect of the entire program. People can’t work harder and there are no better people to hire. The only option we have is to create an organizational structure that functions more efficiently than other programs, if we want to improve faster than they’re improving. That’s why a multidisciplinary team approach is important. It’s literally the only way to compete at this level.”
How does the layout of the new Heart Center help facilitate improved interaction?
“Architecture influences culture. It can enhance or detract from it. Locating cardiology, cardiac surgery, anesthesia, perfusion, the advanced practice providers and our administrative staff in one environment helps make magic. Having everyone in close proximity on the same floors is enormously beneficial for our patients and our care providers.”
You have an active translational research background. Will you continue to build on that?
“I want to continue my own research, but my main objective here is to support other clinician’s translational science efforts throughout the Heart Center. I’ve found that if you get a team together, find resources and focus on a target, you can produce powerful results. My role is to support an environment where multidisciplinary teams routinely get together, target specific areas and create impact. I think of it as translational science ‘one step removed’. I think that’s one of the reasons I’m here.”
What’s something you want people reading this to know about the leadership team’s vision for the Heart Center?
“I want people to know that the Heart Center leadership is dedicated to creating a shared stewardship model, through which we work together to identify specific targets, pool our resources and act upon those targets as a unified group. The model makes collaboration the expectation rather than the occasional nice outcome. In most other institutions, collaboration can happen; there’s nothing to restrict it. But if it doesn’t happen, it’s a silent failure and a missed opportunity.
“Here, we have a group of leaders that is accountable to see that our resources are deployed in a meaningful way that drives change. This creates the dynamic that is necessary to provide that Olympic level of care. If the patient is truly our focus, then every little thing we do here has to be better. Everything has to keep improving. And every single person in the Heart Center has a role and the potential to influence how we extend our lead and, more importantly, how we can improve care for our patients.”
Time for rapid fire: What’s your favorite film?
“The Year of Living Dangerously.”
Favorite sport?
“I don’t really have a favorite. I appreciate a good contest, regardless of the sport.”
Favorite place you’ve traveled?
“Thailand.”
What are you listening to right now on the way to work?
“NPR.”
Beatles or Rolling Stones?
“Tough one! It’s a toss-up. Depends on my mood.”
Caldarone is an internationally recognized leader in congenital heart surgery and most recently served as surgeon-in-chief at The Hospital for Sick Children in Toronto. He received his undergraduate degree from Johns Hopkins University and his medical degree from Columbia University, and he completed his general surgery and cardiothoracic surgery residencies at Beth Israel Deaconess Medical Center/Harvard Medical School. He also completed a fellowship in congenital heart surgery at The Hospital for Sick Children. Caldarone is a member of the American Association for Thoracic Surgery, the Society of Thoracic Surgeons and the Congenital Heart Surgeons’ Society. His specific research interests include the role of apoptosis related mitochondrial dysfunction and remote ischemic preconditioning as mediators of reperfusion injury. Most recently, Caldarone has focused on pulmonary vein stenosis and tissue engineering of pulmonary valves.



























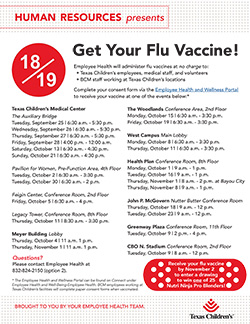 Flu season is almost here! While a record breaking 91 percent of our employees received their flu vaccine in 2017, we continue to strive to make the flu vaccination program even more successful. This year we have a lot of exciting new plans to share with you, such as an increased amount of flu vaccination events across the organization and a new online process for employees to submit proof of vaccinations. As a way to encourage our workforce to get vaccinated earlier in the season, all staff who receive their flu vaccine by Friday, November 2, will be entered into a drawing to win one of 25 Nutri Ninja Pro Blenders.
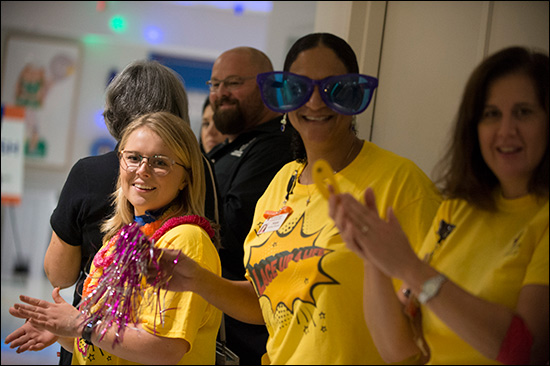
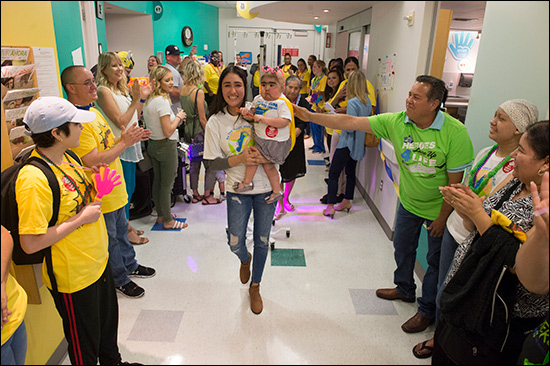
Flu season is almost here! While a record breaking 91 percent of our employees received their flu vaccine in 2017, we continue to strive to make the flu vaccination program even more successful. This year we have a lot of exciting new plans to share with you, such as an increased amount of flu vaccination events across the organization and a new online process for employees to submit proof of vaccinations. As a way to encourage our workforce to get vaccinated earlier in the season, all staff who receive their flu vaccine by Friday, November 2, will be entered into a drawing to win one of 25 Nutri Ninja Pro Blenders. As part of National Childhood Cancer Awareness Month, Texas Children’s Bone Marrow Transplant Unit (BMT) was transformed for a few hours last week into a full-fledged parade route – music, costumes and all.
As part of National Childhood Cancer Awareness Month, Texas Children’s Bone Marrow Transplant Unit (BMT) was transformed for a few hours last week into a full-fledged parade route – music, costumes and all.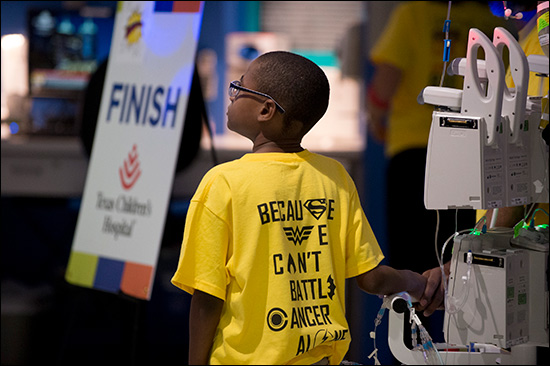
















 Imagine you’re the parent of a newborn with an arm injury. During your admission you’re told not to move the arm and to protect it all times. Now imagine coming back for your clinic appointment and hearing that it’s time to start moving the arm at home – unsupervised. For parents of children with brachial plexus birth palsy, this moment can be daunting.
Imagine you’re the parent of a newborn with an arm injury. During your admission you’re told not to move the arm and to protect it all times. Now imagine coming back for your clinic appointment and hearing that it’s time to start moving the arm at home – unsupervised. For parents of children with brachial plexus birth palsy, this moment can be daunting. Through dedication, hard work, research and partnership, Texas Children’s Newborn Center has lowered its rate of a serious lung condition in premature infants by more than 13 percent over the past year.
Through dedication, hard work, research and partnership, Texas Children’s Newborn Center has lowered its rate of a serious lung condition in premature infants by more than 13 percent over the past year.