Dr. Jordan Orange, vice chair of research in the Department of Pediatrics, announced the winners of the 2016 Pediatric Pilot Awards Research Grant Program. Ten research applications were chosen by review committee members to receive grant funding in the amount of up to $50,000 for their projects.
Dr. Jordan Orange, vice chair of research in the Department of Pediatrics, announced the winners of the 2016 Pediatric Pilot Awards Research Grant Program. Ten research applications were chosen by review committee members to receive grant funding in the amount of up to $50,000 for their projects.
The Pediatric Pilot Awards Research Grant Program provides initial start-up “seed funding” to support research projects. This grant program provides opportunities for new or less established researchers as well as experienced researchers who desire to expand their area of research. The grant projects are awarded based upon their scientific merit and the potential to generate the initial data necessary for a successful grant application submission to the National Institutes of Health or other external, peer-reviewed funding mechanisms.
The pilot award program is a collaborative effort between Texas Children’s Hospital and its academic partner, Baylor College of Medicine.
Congratulations to the following 2016 pilot grant awardees. View the names below to learn more about the research project being funded.
 Saurabh Agarwal, Ph.D.
Saurabh Agarwal, Ph.D.
Pediatrics – Hematology/Oncology
Epigenetic targeting of neuroblastoma cancer stem cells
More than half of the patients with high-risk neuroblastoma (NB) will relapse despite intensive multimodal therapy. Treatments for these patients are challenging due to disease heterogeneity, drug resistance, and toxicity. Thus, novel effective therapies are urgently required to specifically target those tumor cells which escape initial treatment and regenerate chemotherapy resistant recurrent disease.
We identified a G-CSF receptor expressing (CD114+) neuroblastoma cancer stem cell (CSC) subpopulation that is drug resistant, drives metastasis and may cause drug resistant relapse. These highly tumorigenic CSCs are distinguished by specific epigenetic alterations that lead to the expression of specific stem cell genes and maintenance of neuroblastoma CSCs.
We found that epigenetic modifiers MLL1 and JMJD3 increase the expression of G-CSF receptor gene (CSF3R) in NB CSCs by maintaining active histone modifications. Our pre-clinical studies show that blocking these epigenetic modifiers with specific small molecule inhibitors leads to neuroblastoma tumor regression and blockage of metastasis in vivo.
This pilot award will further enable us to test novel dual therapeutic approach by combining epigenetic inhibitors with standard chemotherapy for targeting both stem and non-stem neuroblastoma subpopulations. These studies will define specific epigenetic mechanisms contributing to the maintenance and tumorigenicity of NB CSCs, and pave the way for further clinical translation of our findings to block NB CSC-driven relapse and to advance a novel curative approach to neuroblastoma.
 Wendy Allen-Rhoades, M.D.
Wendy Allen-Rhoades, M.D.
Pediatrics – Hematology/Oncology
Validation of a plasma microRNA panel as a biomarker for osteosarcoma
Osteosarcoma is the primary bone cancer in children and young adults. Currently, there are no reliable, non-invasive biological markers to detect the presence or progression of disease, assess therapy response or provide upfront prognostic insights. MicroRNAs (miRNAs) are evolutionarily conserved, stable, small non-coding RNA molecules that are key post-transcriptional regulators and are ideal candidates for circulating biomarker development due to their stability in plasma, ease of isolation and the unique expressions associated with specific disease states.
In our previous work, we analyzed more than 750 plasma miRNAs from a genetically engineered mouse model of osteosarcoma and identified a diagnostic panel of four plasma miRNAs. This diagnostic panel was able discriminate healthy from diseased animals. Subsequent analysis of 70 human patient samples corroborated these results and the diagnostic panel could discriminate healthy patients from patients with osteosarcoma. Furthermore, low plasma levels of miRNA-214 in metastatic patients at time of diagnosis were prognostic and conveyed a significantly better overall survival.
With the funding from the Pediatric Pilot Award, we will continue the necessary steps to fully validate this novel biomarker by completing validation of the diagnostic and prognostic miRNA biomarkers in 200 additional human samples. The long-term goal of this project is to test these new biomarkers in a prospective clinical trial.
 Sara Anvari, M.D.
Sara Anvari, M.D.
Pediatrics – Immunology, Allergy and Rheumatology
Defining biomarkers of successful peanut oral immunotherapy
Peanut allergy is one of the most common causes of severe and fatal allergic reactions related to food. The prevalence of peanut allergy has nearly tripled in the last 20 years and current standard of care for peanut allergy is strict avoidance of peanuts and ready access to emergency medications. While recent research has demonstrated that early introduction of peanuts, instead of avoidance, during infancy can greatly reduce the risk of a peanut allergy, this strategy is not applicable to individuals who have already developed an allergy.
For older children, teens, and adults, peanut oral immunotherapy (pOIT) is one method by which peanut allergies can be treated through step-wise introduction of peanut protein. This introduction is an effort to manage and reduce the allergic reactions in patients. However, how pOIT alters patients’ immune systems to recognize peanut protein as benign instead of “dangerous” (the nature of severe allergy) is poorly understood. Additionally, biomarkers, or testable indicators of efficacy, for pOIT success in a given patient are also still unknown at this time.
Most current research is focused on how pOIT modifies a white blood cell population, called T regulatory cells, which help control the severity of inflammation caused by immune reactions inside the human body. But T regulatory cells are just one end point of a larger set of immune reactions to pOIT. My research program will focus upstream of T regulatory cells on another population of white blood cells, called dendritic cells, which can communicate with and modify T regulatory cell, as well as several other types of white blood cells.
Specifically, the research award will help (1) identify biomarkers to predict a patient’s success (i.e. peanut tolerance) or failure (i.e. persistent peanut allergy) early in the course of pOIT, without waiting to complete three years of therapy; (2) development of targeted therapies for peanut allergic individuals aimed at altering dendritic cell populations to better modulate T regulatory populations which aid in the reduction of severe inflammatory reactions which make peanut allergies so life threatening.
 Eveline Barbieri, M.D.
Eveline Barbieri, M.D.
Pediatrics – Hematology/Oncology
Targeting MYCN-amplified neuroblastoma through RORa activation
The MYCN oncogene is a transcription factor frequently upregulated in high-risk neuroblastoma, which is profoundly involved in neuroblastoma initiation and progression. Thus, strategies antagonizing MYCN activity are a vital need in neuroblastoma therapy and the focus of this proposal.
Our laboratory has discovered that MYCN-driven neuroblastoma has an increased dependence on glutamine and lipid metabolism. Recent findings in other tumor types suggest an important link between these metabolic pathways and the circadian clock, which is disrupted in aggressive malignancies.
This led us to investigate how MYCN oncogenic signaling, circadian clock, and neuroblastoma metabolic tumor reprogramming are interrelated. Intriguingly, we have found that RORα signaling, a central component of circadian clock, is lost in MYCN-amplified neuroblastoma and this contributes to aberrant tumor proliferation.
Our specific aims will: 1) determine the metabolic programs activated by RORα in MYCN-driven tumors, and 2) determine the in vivo anti-tumor effects of RORα reactivation in pre-clinical neuroblastoma models. These studies will offer insights into critical molecular and metabolic alterations, which will provide new and more sensitive targets that could be strategically deployed with currently available therapies to treat this highly aggressive disease. Moreover, many enzymes in this pathway are amenable to small molecule inhibitors and therapeutic targeting of RORα-mediated metabolism is moving to the clinic.
 Jenny Despotovic, D.O.
Jenny Despotovic, D.O.
Pediatrics – Hematology/Oncology
Genetic variants and gene expression patterns in acute and chronic immune thrombocytopenia
Immune thrombocytopenia (ITP) is an autoimmune disorder and one of the most common causes of low platelets in children. Twenty-five percent of affected children develop chronic ITP and some have significant morbidity and mortality. Currently, it is impossible to predict an individual patient’s clinical course and likelihood of spontaneous remission at the time of diagnosis.
Identification of children more likely to develop chronic ITP at diagnosis would improve treatment decisions and could also help identify important mechanisms of disease that could lead to more tailored treatment. Based on strong preliminary data produced in our laboratory, we believe that acute and chronic ITP are distinct diseases that can be distinguished at diagnosis; and specific genetic changes and gene expression differences influence the development of chronic ITP.
In our study, we are collecting DNA at enrollment on all patients with ITP, as well as RNA on patients with acute ITP at the time of diagnosis and at the time of disease resolution. For patients with chronic ITP, we are obtaining RNA at several time points. We will use the most current sequencing technologies to look for changes that may help explain differences between these two disorders with the eventual goal of identifying markers that could be used to distinguish the two disorders at diagnosis so that we could determine how to best approach each patient.
 John Hollier, M.D.
John Hollier, M.D.
Pediatrics – Gastroenterology
Efficacy of pre-recorded guided imagery session on pediatric gastrointestinal pain disorders managed in primary care
Up to 20 percent of school-age children and adolescents throughout the world are afflicted by recurring abdominal pain that cannot be explained by routine medical laboratory tests or procedures. These children miss more school and rank their general well-being much lower than their healthy counterparts. These disorders also may be associated with psychological distress like anxiety and depression.
One of the most effective treatments for these “functional gastrointestinal pain disorders” (FGIDs) fall under the category of cognitive behavioral therapy. However, access to this type of therapy often is not available due to lack of insurance coverage and/or scarcity of trained healthcare professionals.
Researchers have previously demonstrated the success of guided imagery, a type of cognitive behavioral therapy in treating FGIDs. Guided imagery can be delivered via using compact disc players so that patients can receive therapy at home. Our goal is to find out if audio-recorded guided imagery can be used to treat FGIDs when children are seen in the primary care setting (i.e., by their pediatrician or nurse practitioner). If so, we would be able to get treatment to these children sooner and likely decrease the need for them to be referred to a specialist (gastroenterologist). Our long term research goal is to use mobile cost effective technologies to improve the clinical care of patients with FGIDs and other pediatric diseases.
 Andrew Landstrom, M.D.
Andrew Landstrom, M.D.
Pediatrics – Cardiology
The role of junctophilin-2 in the regulation of cardiac nodal tissue
Diseases that impact the nodal tissue of the heart, such as the heart’s pacemaker, can be life-threatening. Children can suffer from these arrhythmias following surgery, through inheritance within families or for no identifiable reason. These arrhythmias can cause fainting, inability to play with the same energy as other children, or even death from collapse of the circulatory system. Despite how serious nodal disease can be, little is known about how these cells beat and how misbeats can occur. Since basic science has limited understanding of this specialized tissue, the therapies levied against nodal disease are toxic and can be ineffective.
A major reason for the lack of specialized therapies is the absence of experimental models which accurately reflect the arrhythmia. We have created an unparalleled mouse model with cardiac nodal disease that can be molecularly triggered to have arrhythmias from the nodal tissue of the heart. This mouse hosts a molecular switch which allows exposure to a pharmacological trigger to decrease the amount of a protein named junctophilin-2 (Jph2) specifically in the heart.
We have previously shown that reduction in the normal amount of Jph2 in the muscle cells of the heart causes calcium to leak into the cell. This causes a loss of contractile force and cardiac failure. We have also found that human mutations in the gene which encodes Jph2 can lead to cardiac hypertrophy as well as atrial fibrillation. All of these diseases are associated with early, and sometimes sudden, death. We have recently found that expression silencing of Jph2 specifically in the nodal tissue results in a rapid resting heart rate and an arrhythmia known as accelerated junctional rhythm. Our early studies have given strong evidence that this mouse has nodal disease that is very similar to many of the children which suffer from nodal dysrhythmias.
With support from pilot research grant, we hope to delve into the physiology of the cardiac pacemaker and to discover the molecular causes of nodal arrhythmias. We believe that the same calcium signaling that becomes perturbed in the muscle cells of the heart may be to blame for these arrhythmias. Careful interrogation of this possibility, and dissection of the molecular underpinnings of this mouse’s arrhythmias, will offer the first insights into the nodal diseases which remain unexplained and ineffectively treated.
 Jennette Moreno, Ph.D.
Jennette Moreno, Ph.D.
Pediatrics – Nutrition
Assessment of differences in children’s circadian rhythms during the school year and summer vacation
Consistent evidence indicates that school age children demonstrate improvements in their weight status during the school year, yet gain substantial weight during summer. These summertime increases in body mass index (BMI) increase children’s risk for becoming overweight or obese. Further, children at risk for developing chronic health conditions associated with obesity are more likely to demonstrate increases in BMI during summer. Preventing increases in children’s weight during summer may be an important opportunity to address the obesity epidemic in children.
Obesity is conventionally considered a problem of imbalance in energy intake (diet) and expenditure (physical activity/sedentary behavior). There is growing awareness of the role of sleep and circadian rhythms in the development of obesity, yet differences in children’s sleep and circadian rhythms during the school year and summer have not been examined.
Circadian rhythms are internal processes present in all living things that operate on a roughly 24 hour cycle. Behavioral rhythms such as the timing of meals and going to bed and waking up at a consistent time are some of the behaviors known to promote stable circadian rhythms. Changes in sleep and behavioral rhythms may result in disruption of circadian rhythms. Because summer vacation is associated with changes in children’s sleep and behavioral rhythms, the school year and summer vacation paradigm offer an important opportunity to expand our scientific understanding of the role of disruptions in sleep and circadian rhythms on the development of obesity in children.
Little is known about differences in children’s sleep and circadian rhythms during the school year and summer. With the current proposal, we plan to address this gap in scientific knowledge by measuring differences in children’s sleep and circadian rhythms during the school year and summer. We will assess whether differences in sleep and circadian rhythms are related to changes in children’s weight during the school year and summer. These data will may lead to novel approaches to the prevention of obesity in children.
 Robin Parihar, M.D.
Robin Parihar, M.D.
Pediatrics –Hematology/Oncology
Testing a novel non-invasive method to assess efficacy of tumor microenvironment-directed immune therapy
Some children with cancer have solid tumors, or collections of abnormally growing cells, within their organs. These collections are made up of mostly cancer cells, but also of accessory cells that help the tumor hide from the body’s immune system and grow – collectively called the tumor microenvironment. Our laboratory created a new type of immune therapy to specifically target and destroy these accessory cells found within the tumor microenvironment so that they can’t help the cancer grow.
One of the main problems for testing our immune therapy in patients with solid tumors is that we can’t detect these accessory cells without performing a biopsy procedure of the tumor inside the body. In order to detect the accessory cells in patients at many different times during their therapy, we would have to perform repeated invasive biopsy procedures, which come with additional risks and costs. There is currently no non-invasive method by which to determine the effectiveness of therapies that target the tumor microenvironment. If strategies targeting the tumor microenvironment are to be tested in humans, non-invasive methods will need to be developed to evaluate their effectiveness, thereby circumventing the need for repeated invasive biopsies.
Our project involves the creation and testing of a new type of CAT scan that can indirectly detect the accessory cells of the tumor microenvironment. If successful, our new CAT scan can be used to detect changes in the number of accessory cells in patients receiving our new immune therapy, without the need for repeated invasive, risky, or costly procedures. This new CAT scan can be used in clinical trials of other immune therapies as well and may be applied to both children and adults with cancer. The long term goal of the project is to develop a clinical imaging tool that will allow doctors to follow changes within the tumor microenvironment induced by immune therapies.
 Sarah Sartain, M.D.
Sarah Sartain, M.D.
Pediatrics – Hematology/Oncology
The linkage between hemostasis-thrombosis, complement, and inflammation in the pathophysiology of thrombotic microangiopathy
The goal of our research is to improve the health of patients with thrombotic microangiopathy, a group of disorders that cause anemia, low platelets, clots in the blood vessels, and blood vessel damage of the brain, heart, and kidneys. The mechanisms of small blood vessel damage in thrombotic microangiopathy are not precisely defined.
We will investigate the means by which thrombotic microangiopathy causes blood vessel injury and organ damage. We believe that the immune system is involved in the process of vessel injury in thrombotic microangiopathy. This is based on previous work showing that components of the immune system known as the “alternative complement pathway” bind to, and become activated on, long and sticky von Willebrand factor (VWF) strings secreted from blood vessel walls. These VWF strings normally attract platelets to initiate blood clot formation. We intend to determine if activated alternative complement components on these strings contribute to blood vessel injury. We will also determine if a powerful molecule produced during inflammation (known as “tumor necrosis factor”) controls activation of the alternative complement pathway on the VWF strings, contributing to heart, brain, and kidney blood vessel injury.
Our proposed research has long-term biomedical significance because determining the mechanisms of blood vessel/organ injury in thrombotic microangiopathy will lead to the development of therapies to improve the outcomes in this disorder and may be applicable to more common types of blood vessel injury in the general population.
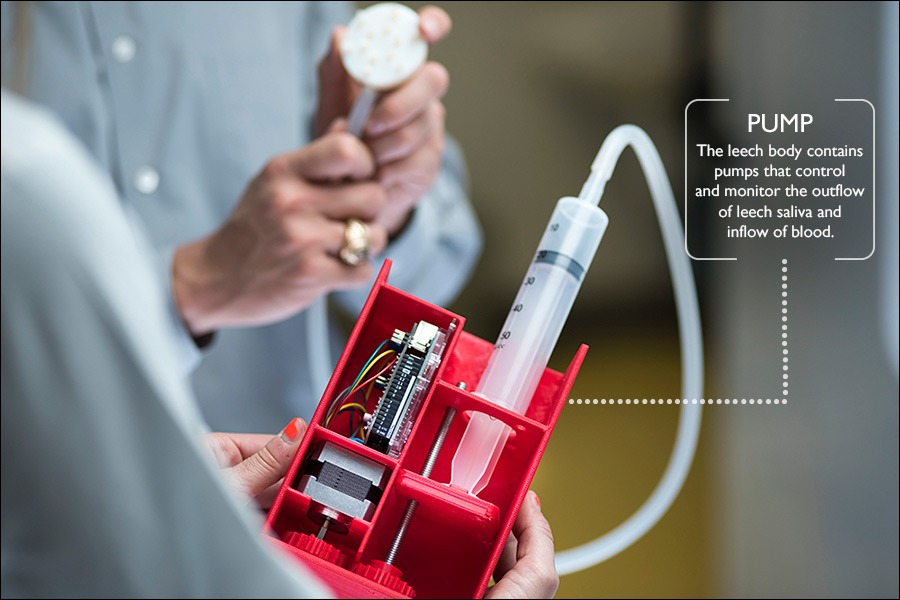
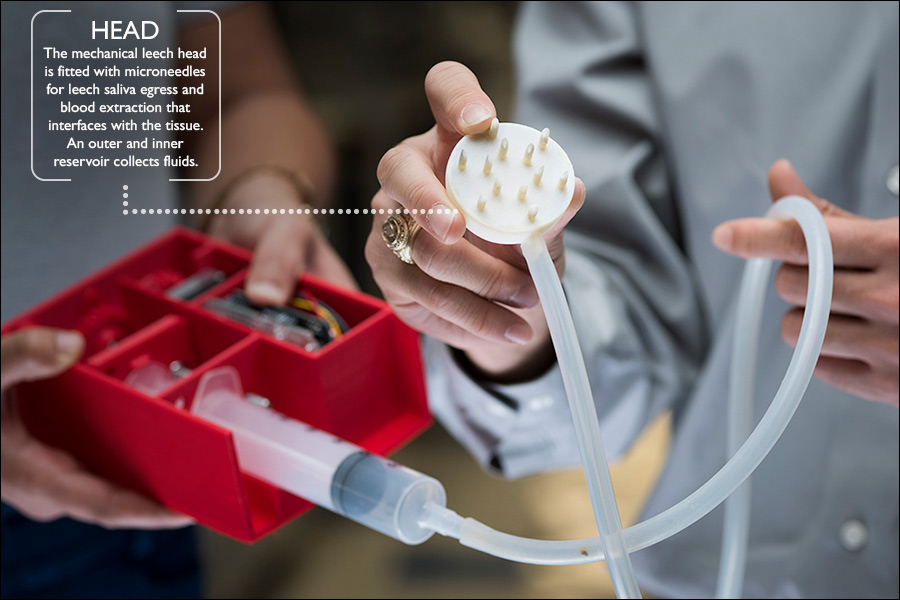
 Have you ever swam in a lake or trudged through swampy waters? If so, you probably have encountered leeches during your outdoor adventures. These worms have been used in human medicine for centuries because of their anesthetic, anti-inflammatory and tissue healing properties.
Have you ever swam in a lake or trudged through swampy waters? If so, you probably have encountered leeches during your outdoor adventures. These worms have been used in human medicine for centuries because of their anesthetic, anti-inflammatory and tissue healing properties.