
As a new school year begins, Denise Tanner-Brown shares helpful tips to prepare parents and children for virtual learning at home during COVID-19. Read more
As a new school year begins, Denise Tanner-Brown shares helpful tips to prepare parents and children for virtual learning at home during COVID-19. Read more

As children across Texas head back to school this month and next, Texas Children’s is preparing for a potential spike in COVID-19 cases. Although it is unclear what will happen when kids return to class, there is a chance that more people will contract COVID-19 due to increased exposure to the virus.
Denise Tanner-Brown, assistant vice president of Community and Ambulatory Nursing, said she is cautiously optimistic considering many schools are starting back virtually, but that no one knows what the next step might be and how that will affect the situation.
“We are standing ready for a second wave of cases and are not letting down our guard,” Tanner-Brown said. “As patient volumes decrease, we have a deactivation strategy where we can temporarily close down units. But, we also have an activation strategy in place where we can turn it back on really quickly should the situation change.”
Critical Care Director of Nursing Shannon Zerber said one of the things Texas Children’s has done well throughout the pandemic that’s reduced the stress of potential surges is adequate planning for space and staff.
A team of experts from across the organization has a tri-campus multitier plan that lays out multiple levels of response. The plan starts with sending patients to the Special Isolation Unit at Texas Children’s Hospital West Campus. Additional beds dedicated to COVID-19 patients are designated at Texas Children’s Hospital in the Medical Center Main Campus, including 13 acute care beds, and six additional ICU beds.
“As our COVID-19 volumes change at Texas Children’s, in Houston and the region, we adapt and flex to demand,” Zerber said. “There is a patient placement group that meets routinely to look at the latest data, so we are ahead of things, not behind. We are anticipating what will happen next.” As a result, Zerber said “everyone is prepared for a spike when school goes back, especially face to face. We all hope it won’t happen but we are ready if it does.”
Dr. Amy Arrington, medical director of the SIU, said the biggest surge Texas Children’s has seen so far was at the end of June and the beginning of July. During that time, all 18 beds in the dedicated biocontainment unit were full and patients were also being cared for at the Medical Center campus.
Since then, the number of COVID-19 patients has dropped, but there has been an increase in the number of patients with multi-system inflammatory syndrome (MIS-C), a delayed inflammatory response to COVID-19 that typically presents four to six weeks after exposure. The syndrome is typically seen in children and teenagers and has varying effects on vital organs, including the heart. Arrington said although the condition is rare, clinicians across the nation are seeing an uptick in cases and that this trend could continue as more children head back to school and are potentially exposed to and contract COVID-19.
Caring for patients with MIS-C takes a tremendous amount of resources and expertise as many patients require stays in the intensive care unit, some of whom need specialized treatment such as extracorporeal membrane oxygenation (ECMO), a treatment that uses a pump to circulate blood through an artificial lung back into the bloodstream.
Texas Children’s has the resources and the expertise to care for these patients. We have intensive care specialists, cardiologists, surgeons, and specialists in rheumatology, infectious diseases and immunology investigating and treating the children as aggressively as needed to ensure they have the best possible outcome.
Chief of Critical Care Dr. Lara Shekerdemian, who has been directly involved in the organization of the intensive care of the 30 plus MIS-C cases at Texas Children’s throughout the pandemic, said Texas Children’s has the capacity to handle a surge of these patients even if it means using areas that aren’t currently being used. Although she said it is unlikely we will see an exponential growth in the number of cases of MIS-C, Shekerdemian emphasized that the capacity is there to care for all those who need the specialized care Texas Children’s can provide.
Arrington agreed and said “So far, space and staffing have never been an issue due to adequate planning and dedicated staff willing to show up for countless extra shifts, work as a unified team and generally go above and beyond. But, we must remain vigilant in our prevention and safety measures.”
Dr. Judith Campbell, medical director of Infection Control and Prevention, added that clinicians at Texas Children’s and other medical institutions from across the world are in a much better position to care for COVID-19 and MIS-C patients than they were in March when the pandemic began.
“We have good evidence now about how to care for patients safely,” Campbell said. “We also have a better supply of personal protective equipment, which makes clinicians and staff feel safer when they are caring for a positive patient.”
Staying on top of the latest research, looking at where we can do better and remaining steadfast in our dedication to our safety measures and protocols, however, are key to our continued success, Campbell said, adding that there is no room to lessen our determination in this pandemic.
Texas Children’s remains committed to providing the safest environment for our patients, families and employees. Since the beginning of the pandemic, we have done an excellent job at keeping people safe while continuing to be there for our patients and deliver top notch care.
Three safety measures that have been implemented across our system and that work very well revolve around screening, social distancing and wearing the proper personal protective equipment. We are constantly adapting and improving these efforts as the situation progresses and changes, but believe we have established a good foundational practice that will be part of our organization for some time to come.
As a reminder, everyone who walks into one of our facilities is stopped and screened for symptoms of COVID-19. Patients, family members and employees alike must fill out a questionnaire about any current symptoms they might have and any recent trips they might have taken. The screening process also includes a temperature check. Months ago, we invested in thermal imaging cameras at our three hospitals to expedite the process and to make it safer for our employees who are administering the screenings.
When on our campus or in any of our facilities, we ask patients, family members and even our own employees to please keep a safe distance of approximately 6 feet from others whenever and wherever possible, including waiting in line and riding in our elevators. We have placed signs and stickers across the system to help keep social distancing top of mind.
Wearing a mask is a must if you want to visit one of our facilities. Patients, family members, visitors and employees are issued a hospital-grade mask after being screened at one of our screening stations. Providers working in certain areas of our system wear additional PPE such as an N-95 mask, a procedure mask, goggles and/or an isolation gown depending on their risk level.
We also have instituted visitor restrictions, video and drive-through visits, precheck-in and online appointment and payment via MyChart, and curbside pharmacy pickup to mitigate any potential exposure to COVID-19 and to alleviate people’s worries about coming to one of our facilities for care.
We have robust testing capabilities and the nation’s largest pediatric primary care network in the nation standing on the front lines of this pandemic triaging patients who might have the virus and helping care for those who do. Texas Children’s Pediatrics is also helping administer COVID-19 tests at our testing sites across the organization and they are continuing to administer much-needed wellness visits and routine vaccines, including the flu vaccine, which will be more than ever for people to receive.
“We have been thoughtful and careful in our planning so that we can turn on a dime if we need to,” said Texas Children’s Pediatrics President Kay Tittle. “Throughout this pandemic, we have figured out how to be more flexible to meet the needs of our families. This will continue to be key in order for us to stay the course and to face whatever comes next.”
Shekerdemian said testing will be extremely important when school opens in order to slow the spread of the virus. It is imperative, she said, that people are honest with themselves and others when they don’t feel well.
“Don’t brush things aside,” Shekerdemian said. “If you (or your family member) don’t feel well, then call your physician and if necessary, isolate yourself and get a test.”
Campbell agreed and said the fall will definitely present an interesting chapter in the story of COVID-19 as it overlays other virial infections that occur commonly in the fall and winter months.
Texas Children’s continues to work hard with our vendor and community partners to implement new programs and opportunities to help lessen disruptions to our team members. As a reminder, check out this guide, which includes information on various topics related to schooling such as discounts, child care, distance learning and much more. Read more

The Child Life team has created buttons personalized with employees’ faces to wear during their shifts. The “face buttons” are intended to help put patients at ease, as they give them a glimpse of the smiling Texas Children’s face beneath the mask and other PPE. The Volunteer Services team is extending this unique and thoughtful effort to all employees and medical staff by hosting “Create your own Face Button” events across the Medical Center Campus next week, with the goal of expanding to other locations soon. Bring your own photo to fit in a 2.5” round button, or come camera ready so your photo can be taken and printed on the spot!
Create your own face button event dates:
Tuesday, August 18
Wednesday, August 19
Thursday, August 20

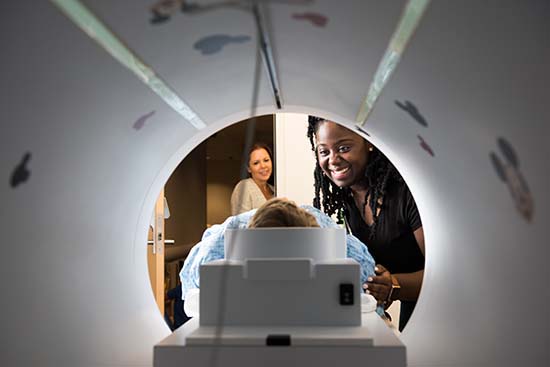
For patients like 5-year-old Legend Pruitt, a visit to the doctor’s office can be a scary place for a child, especially if they don’t know what to expect when they come in for a medical procedure. A few months ago, when Legend had his MRI at Texas Children’s, his mother was surprised by how well he did, and how calm he was during the scan.
“He didn’t move at all because he knew he had to stay still for the MRI,” said Legend’s mother Niayeshua Joseph. “When my son had MRI scans before, he would have to be placed under anesthesia, because he could not stop moving. He is now more comfortable and the noises from the MRI machine don’t bother him.”
In an innovative effort to decrease the need for anesthesia in our MRI patients, Texas Children’s Radiology team bought the organization’s first mock MRI scanner last year thanks to a generous donation from one of our patient families. The mock MRI scanner provides a realistic simulation of what patients can expect before the real exam.
“This innovation allows patients to practice their scan before they enter the real scanner so they can understand their role (to lie still) and are more comfortable with something that is unfamiliar to them,” said Texas Children’s Radiologist-in-Chief Dr. Thierry Huisman. “Mock MR scanner training and familiarity with the MR imaging procedure enhances patient experience, reduces patient and family anxiety, and optimizes patient cooperation which can improve image quality or may allow for imaging without the need for patient sedation or general anesthesia.”
The mock MRI scanner on the fifth floor of Texas Children’s Lester and Sue Smith Legacy Tower, looks and sounds like a real MRI scanner. It has a bed that patients can lie on and travel into a tunnel similar to a real MRI scanner. The MRI scanner makes loud noises while the pictures are being taken. The mock MRI scanner simulates those noises and prepares a child for what to expect before they are scanned using the real machine. One additional advantage is that the mock MRI scanner does not include the “big magnet” and allows patients and families to attend without limitations. Furthermore, the mock MRI scanner does not use costly time as the real MRI unit.
Patients can get prepped with the mock MRI scanner in two ways. If the radiology pre-call nurse identifies a patient through their screening, they can schedule an appointment with a child life specialist several days before their procedure. Patients can also test out the mock MRI scanner immediately before their MRI appointment.
After introducing the mock scanner in July 2019, Radiology has seen amazing conversion results. Since June of this year, 67 patients have used the mock MRI scanner and 39 MRI patients scheduled for general anesthesia were converted to non-sedate procedures.
“We are really excited about our initial success,” Dr. Huisman said. “We are grateful to have this resource available to our patient families, and incredibly grateful to the Cook family’s philanthropic donation to make this all possible.”
Brady and Nancy Cook know first-hand the challenges patient families face when a young child has to undergo an MRI especially for the first time. When their daughter, Alyssa, was in kindergarten, she started having complex partial seizures and was later diagnosed with a brain tumor. The brain tumor was believed to be in the area of the brain where speech is generated but doctors didn’t know for sure unless they performed a functional MRI on her.
“With a functional MRI, the patient has to be awake in the MRI machine and respond to images that flash up on the screen inside the MRI without moving because it would distort the quality,” said Brady Cook. “For that reason, it’s typically not done on 5-year-olds, because they are unable to hold still for an hour and follow instructions like that.”
But everything changed when the couple came across a research study on the use of mock MRI scanners that taught kids how to be more comfortable around the MRI machine to the point where young children could endure it. Out of desperation, they got creative and built a mock scanner in their garage. They used a big refrigerator box, a dolly that you lay on to get underneath a car, a softball mask to simulate the cage that goes over the patient’s head, a school locker sized mirror, age appropriate flash cards, and downloadable sound effects mimicking an MRI machine.
“We practiced this on our daughter so she could get comfortable with the MRI machine,” said Cook. “Soon after, she was able to successfully complete a functional MRI without moving. Her MRI scans showed us that the tumor was nowhere near the area of her brain that generates speech, and therefore the tumor could be removed safely.”
Since the mock MRI scanner helped their daughter, the Cook family wanted Texas Children’s to have the capability of helping patients become more comfortable with the MRI machine. Through their generous donation to Texas Children’s, the family is grateful that the mock MRI scanner is making a positive impact on patients and families.
“As parents who have been through this before and the desperation we felt at the time, we would do anything to ensure patients are comfortable during this process leading up to surgery,” Nancy Cook said. “Now that we have a mock scanner here, we hope that it will continue to give parents and children added comfort and reassurance.”




Many of you know that I have a 7-year-old daughter. She just started the second grade. Having a child this age means I spend a great deal of time baking cookies, going to dance practices and watching Disney movies. One of our favorite Disney productions is “Princess and The Frog,” the 2009 animation about New Orleans native Tiana and her dreams of owning a restaurant.
There is so much to enjoy about “Princess and The Frog” beyond the actual story. One of those things is Disney’s ability to capture elements of the African-American culture and the culture that exists within the city of New Orleans. To appreciate the cultural elements of the movie is to appreciate the movie itself.
I instantly thought about “Princess and the Frog” when we, at The Heath Plan, began to prepare for the launch of a new state-mandated Cultural Competency course. I began to think about the culture of our organization and I realized something. One of the reasons I enjoy working at The Health Plan is because our employee population, provider network and member base is extremely diverse. But most importantly, there is an urgency to understand our diversity and discover how we can leverage it to improve our business.
This new course – mandatory for all Health Plan employees – is a series of training modules covering 15 national cultural competency standards. It is available now through September 30 on HealthStream. The arrival of the course and an overall focus on culture and communication will be celebrated during The Health Plan’s Cultural Competency Week Monday, August 24, through Friday, August 28. A variety of virtual activities will also take place to highlight the importance of the effort.
I am thrilled to see this happening. In my opinion, there is no higher compliment than to acknowledge and seek to appreciate the differences between each other. This acknowledgment and appreciation improves communication, relationships and an ability to meet each other’s needs. This is essentially the definition of cultural competence.
Watch Connect over the next few weeks for stories that dive deeper into the national standards and provide details on how we are striving to uphold them in our daily work.
Hope and grief
The following passage was written by Texas Children’s Chaplain Natalie Peters.
I participated in virtual Respite Rounds hosted by our own Palliative Care team this past week. The topic of discussion was about when grief and hope mingle, and I found myself taken back to a time exactly a year ago when I experienced a heap of grief and hope in just one day. On this particular day, I woke up to news that a patient I had become close to and had been following practically from birth had died.
I was expected to give a prayer at an event later that morning, so I had to set aside my sadness and lead the prayer and interact with families afterward. Despite my grief, there was hope in seeing these families and hearing how much of an impact I had on them during their stay at Texas Children’s.
I went home and let out everything I had been holding in. As I write this now, I still have vivid memories of this day. However, I am looking through a different lens now than a year ago. I can imagine that many of us here at Texas Children’s have had to suppress some kind of grief whether it be tangible or intangible, but that somehow we have hope despite the pain and loss associated with those feelings.
Both grief and hope are complex and can mean completely different things to each of us, especially with many of us grieving the normalcy that once was and hoping for so much to change. Hoping for the trip you took months to plan, hoping for more hours in the day to get all of the new tasks you need to do done, and so on. Sometimes what one person grieves, another hopes for and vice versa. When I think back to that day last year, as hard as it was for me emotionally, it was very much necessary to have both grief and hope.
One of the hardest obstacles I have had to overcome after a death of a patient was coming to the hospital. Finding the strength and courage to enter the unit, walk by the bed space that child had occupied and pause for a moment is often extremely difficult. However, I realize in this world there is always going to be hope and grief.
C.S Lewis writes that “No one ever told me that grief felt so like fear. I am not afraid, but the sensation is like being afraid. The same fluttering in the stomach, the same restlessness, the yawning. I keep on swallowing … There is a sort of invisible blanket between the world and me …”
Yet despite the fear, there is also hope. With hope there is also fear. I am hopeful for this “new normal” yet fearful of what it means moving forward. Normalcies that I once knew like concerts, social gatherings, and traveling will look dramatically different moving forward. But I also hope for them as well because there was so much joy in those moments and experiences.
With the end of the year closer in reach, there are mixed feelings of both grief and hope. Grief of many things this pandemic has robbed us of as well as hope for the new normal and lessons learned from this year. When the lows we feel are hitting us hard, there is always hope. And when there is hope, there is grief. And sometimes you will feel them separately or in some cases, at the same time. This pandemic has me looking at this world in a new lens. I often feel isolated in my grief and have a different outlook as I deal with grief a lot in my work as a chaplain but this year, I feel so many more of you understand what it is to live in this world of both grief and hope.
“Only people who are capable of loving strongly can also suffer great sorrow, but this same necessity of loving serves to counteract their grief and heals them.”-Leo Tolstoy