
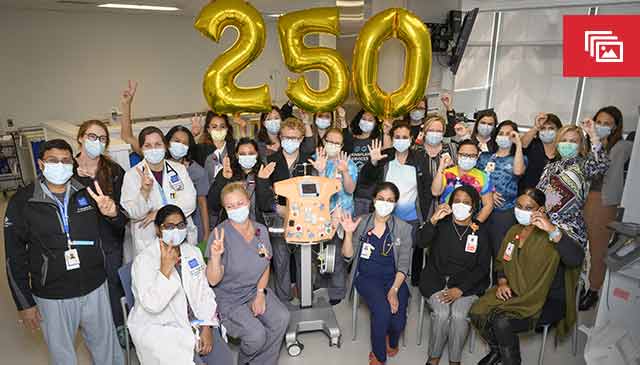
Texas Children’s Hospital is excited to unveil our newly renovated Dialysis & Apheresis Center! Last week, the team officially moved into the new space on West Tower 6 and began treating patients.
The revitalized unit is tripled in size from the original, topping out at over 24,000 square feet with 23 patient care stations. The space is inviting with an abundance of natural light, and patients can enjoy the “Under the Sea” theme complete with wall art and fish tanks. It also features a dedicated patient and family support area, including a large waiting room, family lounge, play zone, and quiet space for nourishment and relaxation.
As the top-ranked program grows in volume and service offerings, leaders felt an expansion plan was needed for outpatient dialysis and apheresis to better meet the unique needs of our patients and families.
“The opening of our new Dialysis & Apheresis Center is a transformational event for the renal service, our patients and their families,” said Chief of Renal Services Dr. Michael Braun. “We are grateful to Mr. Wallace and the Board of Trustees for their commitment to the care of children with kidney disease…these facilities have set a new standard for pediatric dialysis and apheresis units in the United States.”
Click the gallery for more photos of the new Dialysis & Apheresis Center. Ranked #1 in Nephrology by U.S. News & World Report, Texas Children’s is home to one of the largest and most comprehensive pediatric renal services in the world. Click here to learn more.

































 From the time Colton Makow was born, he faced an uphill battle. He spent his first 61 days of life in Texas Children’s Hospital’s Neonatal Intensive Care Unit, and while there, was told by doctors that his kidneys were damaged from lack of oxygen and that he one day would need a transplant.
From the time Colton Makow was born, he faced an uphill battle. He spent his first 61 days of life in Texas Children’s Hospital’s Neonatal Intensive Care Unit, and while there, was told by doctors that his kidneys were damaged from lack of oxygen and that he one day would need a transplant.



